Abnormal Pap Smears
“Many women with
an abnormal Pap smear
mistakenly believe
that they have cancer
If you are young, you are in danger
of being over treated
If you have avoided Pap smears
for a long time you are in danger
of being undertreated
My goal is to see that you
are treated appropriately”
Raymond Lackore MD
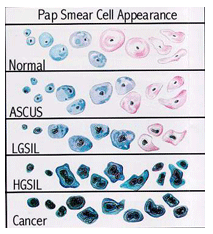
If you have had an abnormal pap smear then your cervix needs to be evaluated for dysplasia. Dysplasia is not cancer, but it can turn into cancer if it is not treated. By proper treatment of dysplasia and by proper follow-up, we can significantly reduce the chances that cancer might develop. Dysplasia may be low grade (LGSIL) or high grade (HGSIL) or if severe, CIS (carcinoma in situ).
TREATMENT OPTIONS:
Watchful waiting – close follow-up
Interval pap smears
Magnification and tissue sampling
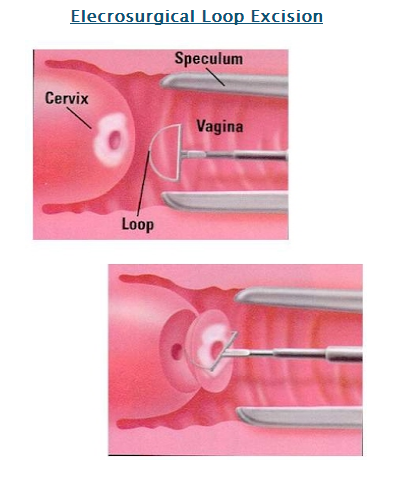
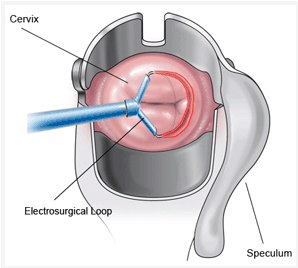
Loop Electrosurgical Excision Procedure (LEEP)
Excision with Scalpel – uncommon
Removal with a laser – less common
Hysterectomy for recurrent High Grade or cancer
Treatment choice depends on the severity of the abnormality, how widespread it is, the patient’s age, childbearing desires, available resources, physician training and patient preference. There are some cases that can (and should) be carefully followed without treatment if the physician and patient are willing.
MARKEDLY ABNORMAL PAP SMEARS REQUIRE A BIOPSY OF THE CERVIX (APPEARANCE BELOW)

CHOOSING THE BEST TREATMENT FOR ABNORMAL PAP SMEARS:
Abnormal pap smears are treated by identifying the area of abnormal cervical tissue and removing it to prevent worsening or spread to other areas of the cervix. There are several approaches to the treatment for cervical abnormalities:
Observation with close follow-up using pap smears and magnification (colposcopy) every 6 months – often favored for adolescents (13-20 years).
Treatment that destroys the abnormal area (called ablative therapy) – for milder non-recurrent problems that are clearly seen (cryosurgery, laser or radiosurgical ball tip electrode).
Treatment that removes the abnormal areas (called excisional therapy) – favored by most physicians for persistent mild changes or initial treatment of moderate/severe changes Loop Excision by Electrosurgery).
Hysterectomy – uncommon except for severe and/or persistent findings/almost always in more mature women.
MANAGEMENT OF ABNORMAL PAP SMEARS
A NEW APPROACH: (For adolescents and young women) the new (more conservative) recommendations for management of mild or low-grade changes is follow-up by Pap smear. Treatment is now particularly discouraged in adolescents. Moderate or severe changes (CIN 2,3 – high-grade changes) now also have the option of being managed by close follow-up with pap smears and colposcopy in adolescents and young women only. These guidelines should never substitute for clinical judgment.
ADOLESCENTS AND YOUNG WOMEN: Adolescents aged 13 to 20 years, and young women are very low risk for invasive cervical cancer. In this age group there is a very high rate (approximately 90%) of the changes going away by themselves within 24 months. Patients with low grade changes should be followed up every 6-12 months with Pap smears or every 12 months with HPV DNA testing. Once 2 consecutive Pap smears are normal then a return to routine Pap smear screening is recommended.
The method I use is electrosurgical removal of abnormal cells (Also known as LEEP). In the past I have used a scalpel or laser but in my hands, for the cases I manage, the electrical loop is more effective than these other techniques. Excision methods have the advantage of producing a specimen that can be looked at under the microscope. Using a scalpel, laser or electrical loop to excise tissue does create a low risk of future pregnancy problems. These include delivering a baby when it is premature and too small. It is therefore extremely important that the surgeon use careful judgment in deciding how much tissue to remove.
 OTHER TREATMENTS: There are no generally accepted nonsurgical (local liquids, creams or gels) treatments for Cervical changes that may lead to future cancer. Several treatments have been tried (Trichloroacetic acid, Aldara) but none has been proven to be as effective as ablation or excision. The decision of which treatment to use for an individual patient depends on the patient’s age, the number of children she’s had, her future childbearing desires, her personal preferences, her prior abnormal Pap smears, her previous treatment history, her history of failing to follow-up, operator experience and being unable to see the cervix clearly with colposcopy (magnification).
OTHER TREATMENTS: There are no generally accepted nonsurgical (local liquids, creams or gels) treatments for Cervical changes that may lead to future cancer. Several treatments have been tried (Trichloroacetic acid, Aldara) but none has been proven to be as effective as ablation or excision. The decision of which treatment to use for an individual patient depends on the patient’s age, the number of children she’s had, her future childbearing desires, her personal preferences, her prior abnormal Pap smears, her previous treatment history, her history of failing to follow-up, operator experience and being unable to see the cervix clearly with colposcopy (magnification).
TREATMENT FAILURES: If after surgical treatment an abnormality is found to still be present at the internal or external margins, then follow-up with Pap smears and endocervical Cytobrush is preferable and repeat conization is acceptable. The treatment failure rate for using either destruction or cutting-out /excisional methods is somewhere between 5 and 15%. Most failures occur within 2 years after treatment. Women with significant conditions that might lead to future cervical cancer remain at increased risk for a prolonged period of time. Because of this follow-up is essential. A number of follow-up protocols have been recommended. The follow-up protocol I prefer is using very carefully collected pap smears (including a tiny brush sampling up inside the cervix every) six months with colposcopy for any abnormalities found.
If a high-grade lesion is persistent or there are other gynecologic problems ongoing then hysterectomy may be considered.
VALUABLE LINKS: